
We are living in a golden age of biology where we can effectively treat and even cure diseases in the liver, lungs, and blood with unprecedented precision. But when it comes to the brain, the door remains shut. For patients with Alzheimer’s, glioblastoma, or Parkinson’s, this biological revolution has felt largely out of reach, and it’s not because we lack the right drugs. We have potent treatments that should work, but we cannot get them onto the battlefield. This is the reality of the Blood-Brain Barrier (BBB), a structure so effective that it has turned the Central Nervous System (CNS) into what scientists have called the “graveyard of drug discovery [1]. But in recent years, the narrative is shifting. We are moving from an era of trying to break through the wall to unlocking the door.
Realizing this shift, however, requires a deeper understanding of the barrier and the development of new tools to navigate it efficiently. As the field shifts toward precision brain delivery, attention is turning to antibody formats that can both unlock new BBB targets and enable efficient therapeutic design. Fully human HCAb-derived VH domains offer a unique combination of stability, manufacturability, and engineering versatility, while their small size enables access to epitopes that are often inaccessible to conventional antibodies. Just as importantly, their affinity can be readily optimized to enhance BBB transcytosis and tissue distribution, creating new opportunities to overcome longstanding barriers in CNS drug development.
To appreciate why these new approaches are necessary and where they can succeed, it is critical to first understand why the BBB is so effective in the first place.
Why the Wall Exists: An Evolutionary Fortification
The brain is a finely tuned electrochemical machine that relies on precise ionic gradients to fire neurons. If it were exposed to the chaos of the general bloodstream, where potassium spikes after you eat a banana, or pH shifts when you go for a run, then our neurons would misfire uncontrollably, leading to seizures and death.

On top of that, many molecules the brain uses as neurotransmitters are made in large quantities in other parts of the body, for example, digesting food (serotonin), fueling muscle metabolism (glutamate), and driving the physical mechanics of the fight-or-flight response (epinephrine). These molecules are equally essential in the brain, but for different reasons. Serotonin stabilizes mood and sleep, glutamate carries electrical signals for learning and memory, and epinephrine sharpens focus. The Blood-Brain Barrier exists to strictly separate these two pools, otherwise the massive reservoirs of stimulatory chemicals circulating in the blood would flood the brain’s synaptic clefts, drowning out rational thought in a sea of biological noise. Finally, the brain is enclosed in a rigid skull and cannot afford any increase in size. An integral role of the BBB, therefore, is to keep the immune system out of the brain to prevent inflammatory responses that could trigger swelling, and this is known as “Immune Privilege” [1].
Nature built this wall to maintain neural homeostasis, and it works exquisitely. Unfortunately, however, it also keeps 98% of small-molecule drugs and nearly 100% of large-molecule therapeutics locked out.
Finding the Key: The Rise of TfR1
While the BBB exists to keep harmful levels of molecules out, it cannot be a terminal blockade. Consequently, a host of Receptor Mediated Transcytosis (RMT) receptors pepper the luminal-facing space to facilitate transfer of vital molecules across the BBB. To synthesize its delicate signaling networks, the brain requires the selective transport of raw amino acid building blocks and essential micronutrients (like iron) across the blood-brain barrier. Iron is a vital micronutrient for the brain, serving as an essential co-factor for generating the massive amounts of cellular energy neurons require, synthesizing key neurotransmitters like dopamine, and producing the protective myelin sheaths that insulate nerve fibers.
TfR1, also known as CD71, is a homodimeric type II transmembrane glycoprotein that plays an indispensable role in cellular iron uptake and metabolism. Highly expressed on the luminal surface of brain capillary endothelial cells (BCECs), TfR1 is the primary gateway for brain tissue to acquire iron from the bloodstream, where the molecule is shuttled across this otherwise impenetrable barrier, tightly bound to the glycoprotein transferrin (Tf). And herein lies a therapeutic opportunity. By mimicking iron’s entry pass, TfR1 antibodies can be engineered into shuttles that hitch a ride via a process called Receptor-Mediated Transcytosis.
Critically, the utility of TfR1 as a BBB shuttle for therapeutic use is underlined by its functional preservation in many neurodegenerative diseases. Other potential therapeutic options for BBB shuttles, such as tight junction proteins and efflux transporters, exhibit dysfunction or reduced expression in Alzheimer’s Disease (AD), which could hamper drug delivery efforts. Expression levels and functional integrity of TfR1 in AD are mostly preserved, however, despite the presence of sustained neuropathology associated with the disease. These attributes have established TfR1 as a bona fide BBB shuttle option.
While clinically approved non-antibody methods are restricted to tiny chemical precursors, single-dose viral vectors, or invasive mechanical disruption, engineered antibodies remain the sole clinically validated architecture capable of safe delivery of large macromolecules into the brain, a milestone definitively proven by the historic regulatory approval of the TfR1-targeted enzyme IZCARGO® [3]. But while the target is not new, the way these shuttles have been engineered has undergone a quiet revolution.
The First Wave: The ‘Affinity Paradox’
Early attempts to use TfR1 were logical but flawed. Scientists assumed that to get more drug into the brain, you needed a stronger binder. But they were wrong. Research pioneered by Genentech revealed an ‘affinity paradox’, where less becomes more. To appreciate this juxtaposition, it helps to understand how TfR1 shuttles its cargo across this ancient barrier.
The first step in the process is the binding of iron-loaded transferrin (or a therapeutic agent designed to mimic transferrin) to TfR1 on the luminal surface of BCECs, which triggers clathrin-coated pit formation and internalization of the receptor/ligand complex into early endosomes. Here, a sudden drop in pH weakens interactions between the receptor and cargo. Cargo that dissociates from the receptor at this point is shuttled into sorting tubules that bud off from these early endosomes. This cargo then crosses the endothelial cytoplasm and fuses with the abluminal membrane, which releases the cargo into the brain interstitium [4].
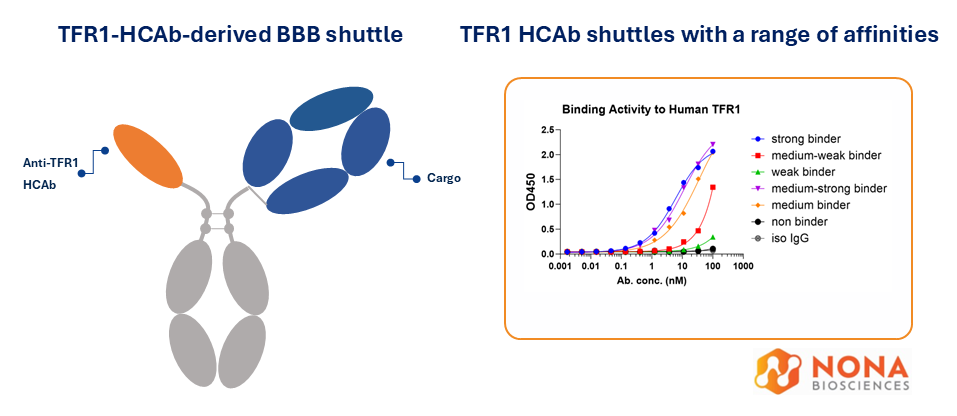
This finely tuned blood-brain cargo conveyor belt requires that therapeutic manipulation of the system be similarly tuned, and antibody affinity is crucial here. Higher affinity or bivalent binding results in antibodies that hold onto TfR1 too tightly and for too long and miss the sorting tubule drop-off point, accumulating instead in endolysosomes where they are targeted for degradation [5]. Of course, TfR1 antibodies with too low affinity don’t bind the receptor properly and are not internalized in the first place. However, moderate affinity or monovalent engagement reduces receptor clustering and increases the fraction of cargo released into tubules to be shuttled across endothelial cell cytoplasm to the brain interstitium [6]. This creates a ‘Goldilocks’ zone of moderate affinity for therapeutic TfR1 BBB shuttle antibodies, which must bind TfR1 tight enough to be captured from the blood, but loose enough to let go once they reach the brain-facing side [7].
The Second Wave: The ‘Pairing Challenge’
Once the biology was understood, the challenge became an engineering one. How do you build a molecule that binds a therapeutic cargo and TfR1, and retains an optimal profile to cross the BBB? Traditional bispecific antibodies require two different heavy and light chains, and mixing them often results in mispairing, creating junk molecules where the wrong light chain pairs with the wrong heavy chain [8].
To bypass light-chain mispairing, developers fused single-chain variable fragments (scFvs) to standard IgG scaffolds. However, stripped of stabilizing constant domains, the synthetic VH-VL interface is thermodynamically unstable and with a propensity to aggregate, requiring artificial cysteine ‘staples’ just to remain intact, while their exposed peptide linkers remain highly vulnerable to proteolytic cleavage in systemic circulation [9]. Conversely, utilizing full Fab fragments as in brain shuttle designs by Genentech, resolves the thermodynamic instability of scFvs but resurrects the light-chain pairing issues, necessitating structural workarounds to prevent chain scrambling. Furthermore, appending a 50 kDa Fab creates a large (~200 kDa) molecule that could restrict its ability to diffuse through the dense brain parenchyma post-transcytosis.
A Refinement: Heavy Chain Only Antibodies (HCAbs)
To escape the structural tug-of-war between fragile scFvs and bulky Fabs the industry utilized single-domain biology, camelid-derived VHH (nanobodies) and structurally similar shark VNAR emerged as compelling alternatives [10]. Pioneered by the National Research Council of Canada (NRC) and specialized biotechs, these shuttles successfully validated the single-domain architecture, driving major ongoing CNS collaborations across Big Pharma, including giants like Biogen, AstraZeneca, Novo Nordisk, and Lundbeck [11]. Conceptually, a single-domain shuttle is an ideal format. Because it naturally lacks a light chain and is inherently small (~15 kDa), it solves many of the issues of scFv and Fab approaches for BBB shuttle design. While many of these single-domain platforms remain in active development, utilizing non-human domains is also not ideal. The humanization process required to prevent immunogenicity in patients can result in loss of the ‘Goldilocks’ affinity range required for optimal BBB shuttle function, thereby requiring multiple further rounds of development to re-tune this affinity.
The Next Generation: Fully Human HCAbs
Why struggle with the humanization process when you can bypass it entirely? This is the paradigm shift offered by fully human Heavy Chain-Only Antibodies (HCAbs) [12] (Janssens et al., 2006). By leveraging transgenic platforms like Nona Biosciences’ Harbour Mice®, protein engineers can generate naturally occurring, fully human monomeric heavy chain only domains directly in vivo. By utilizing a fully human HCAb as the TfR1 targeting domain, developers retain the validated single-domain architecture while eliminating the compounding liabilities of previous formats:
- Enhanced Stability (no scFv staples): eliminates the aggregation and synthetic linker cleavage vulnerabilities of scFvs.
- No Mispairing & Minimal Bulk: HCAbs can be seamlessly appended to any standard therapeutic IgG without complex engineering, while their minimal ~15 kDa footprint maximizes parenchymal diffusion.
- No Humanization Required: Because Harbour Mice® generate fully human sequences from inception, the immunogenicity liability is preemptively resolved.
- ‘Plug-and-Play’ VH Format: HCAbs can be easily fused to existing clinical antibodies, allowing for direct chemical conjugation to create bispecifics without the need to rebuild molecules from scratch, providing a significant advantage for endowing current pipelines and existing batches of clinical material with BBB-crossing capabilities.
Beyond TfR1: Expanding the Transcytosis Toolkit
While TfR1 has served as the trailblazer for receptor-mediated transcytosis, it’s not the only gatekeeper. As CNS pipelines expand to include diverse payloads from large antisense oligonucleotides (ASOs) to complex gene therapy capsids, the industry is realizing that a ‘one-size-fits-all’ shuttle may not suffice. Furthermore, because TfR1 is highly expressed on reticulocytes, developers must engineer their shuttles to navigate this peripheral sink and avoid safety liabilities.
Consequently, the industry is exploring additional transcytosis pathways, including:
- CD98 (CD98hc): The heavy chain of the large neutral amino acid transporter (LAT1). CD98 is emerging as a premier next-generation target because it offers massive transport capacity across the brain endothelium and a potentially differentiated peripheral safety profile [13].
- IGF1R (Insulin-like Growth Factor 1 Receptor): While early approaches faced metabolic liabilities from accidentally activating the receptor, highly refined, strictly monovalent binders are reviving IGF1R’s promise [14].
Crucially, finding a new door does not change the need for a better key. Whether the industry targets TfR1, CD98, or IGFR1, the fundamental biophysical rules of transcytosis remain absolute. If developers attempt to drug CD98 or IGF1R using scFvs, Fabs, or non-human VHHs, they will encounter the same thermodynamic instabilities, mispairing, size, and humanization issues. With Nona Biosciences’ Harbour Mice®, that bottleneck is erased. We can deploy our in vivo engine against CD98, IGF1R, or any newly identified BBB target, and isolate fully human, natively stable single domains ready to be modularly fused as a plug-and-play cassette to any therapeutic payload without the need for humanization, cysteine staples, or complex chain-pairing.
For decades, the Blood-Brain Barrier dictated the limits of neurology, famously earning its title as the ‘graveyard of drug discovery.’ But driven by a deeper understanding of neural homeostasis and the elegant simplicity of fully human single-domain biology, the narrative has changed. We are no longer trying to force the wall to break; we are systematically building the master keys to unlock the brain.
To explore Nona’s fully human VH binders against CD98, IGF1R, or newly identified BBB targets, contact us below to discuss your CNS delivery strategy.
Related Resources
To explore next-generation CAR design and delivery strategies in more detail:
- Download our Poster on Fully Human VH CAR platforms for a concise, visual overview of HCAb-derived VH domains applied in CAR-format screening, functional validation, and targeted delivery workflows
- Read our Blog on Ex Vivo to In Vivo CAR Therapy for insights into how CAR therapies are evolving toward in vivo delivery and expanded therapeutic applications
- Pardridge W. M. 2005. [Link]
- Alahmari A. 2021. [Link]
- Okuyama et al. 2021. [Link]
- Bien-Ly N. et al. 2014. [Link]
- Baghirov H. 2025. [Link]
- Niewoehner J. et al. 2014. [Link]
- Yu Y.J. et al. 2011. [Link]
- Spiess C. et al. 2015. [Link]
- Bhatta P. & Humphries J. 2018. [Link]
- Jovčevska I. & Muyldermans S. 2020. [Link]
- Abulrob A. et al. 2005. [Link]
- Janssens R. et al. 2006. [Link]
- Donnopadlo G. et al. 2024. [Link]
- Shin J.-W. et al. 2022. [Link]
