
Global Landscape of Autoimmune Disease CAR T Clinical Studies
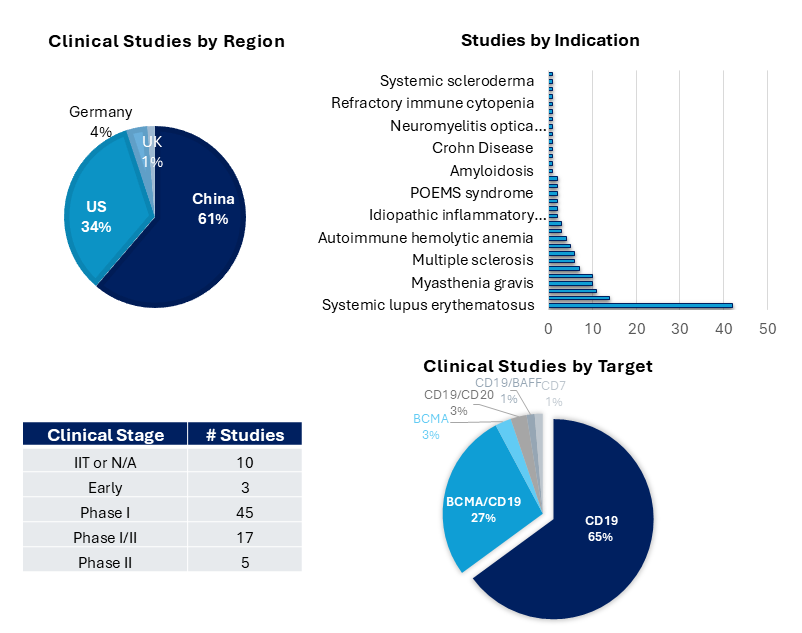
The majority of trials evaluating CAR-T cells in autoimmune diseases are still in early clinical stages and are predominantly conducted in China and the US. These include several Investigator Initiated Trials (IITs) (e.g., NCT06549296, NCT05930314, NCT05859997, NCT05988216, NCT06277427).
IITs provide a versatile clinical mechanism for investigators to explore novel questions, expedite early-stage testing, and generate real-world clinical insights and data to shape future trials.
For CAR-T cell therapies in autoimmune disease, the single biggest advantage of IITs is that they enable rapid, clinician‑driven exploration of immune reset as a completely new therapeutic paradigm, expediting industry timelines, commercial justification, and large‑scale infrastructure. As such, currently, IITs are being leveraged to evaluate safety, tolerability, pharmacokinetics, pharmacodynamics, and preliminary efficacy in various autoimmune disease patient populations.
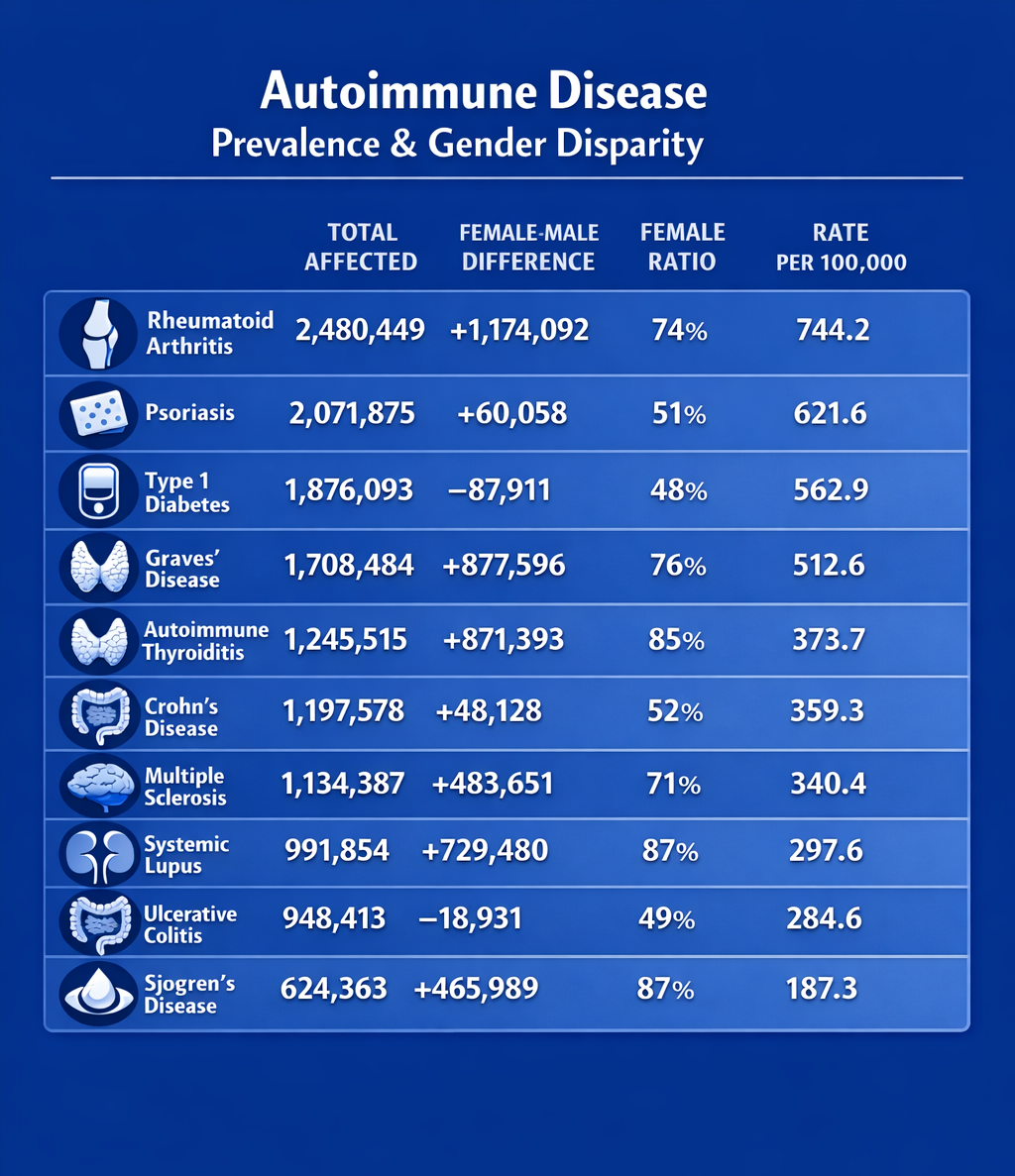
Among both investigator-initiated and clinical trials, systemic lupus erythematosus, lupus nephritis, ANCA-associated vasculitis, myasthenia gravis, and systemic sclerosis figure prominently as the top five most studied indications.
Not surprisingly, given the success of CD19- and BCMA-targeting CAR-T cells in hematological malignancies, these B-cell receptors are leveraged prominently in autoimmune disease. The majority (~65%) and more advanced studies focus on CD19-targeting therapies because CD19 is broadly expressed across B-cell subsets, from pro-B cells to subsets of plasma cells. Nevertheless, as CD19 expression is downregulated in both short-lived and long-lived plasma cells, a substantial number of studies use combined CD19 and BCMA CAR-T cells to deplete plasma cells.
Relevant B-Cell Receptors for CAR-T Cell Therapies

By depleting populations of autoantibody-producing plasma cells that persist for years, this combined approach can enable long-term remission in autoimmune disease patients [2].
Advancing strategies targeting autoreactive B cells
A caveat of BCMA/CD19 CAR-T cell therapies in autoimmune diseases is the resulting widespread B cell depletion, which weakens immune responses and increases susceptibility to infections. Therefore, emerging trends are leveraging two main approaches to more specifically target autoreactive B cells.
Chimeric Receptor Strategies for T Cell Therapies in Autoimmune Diseases
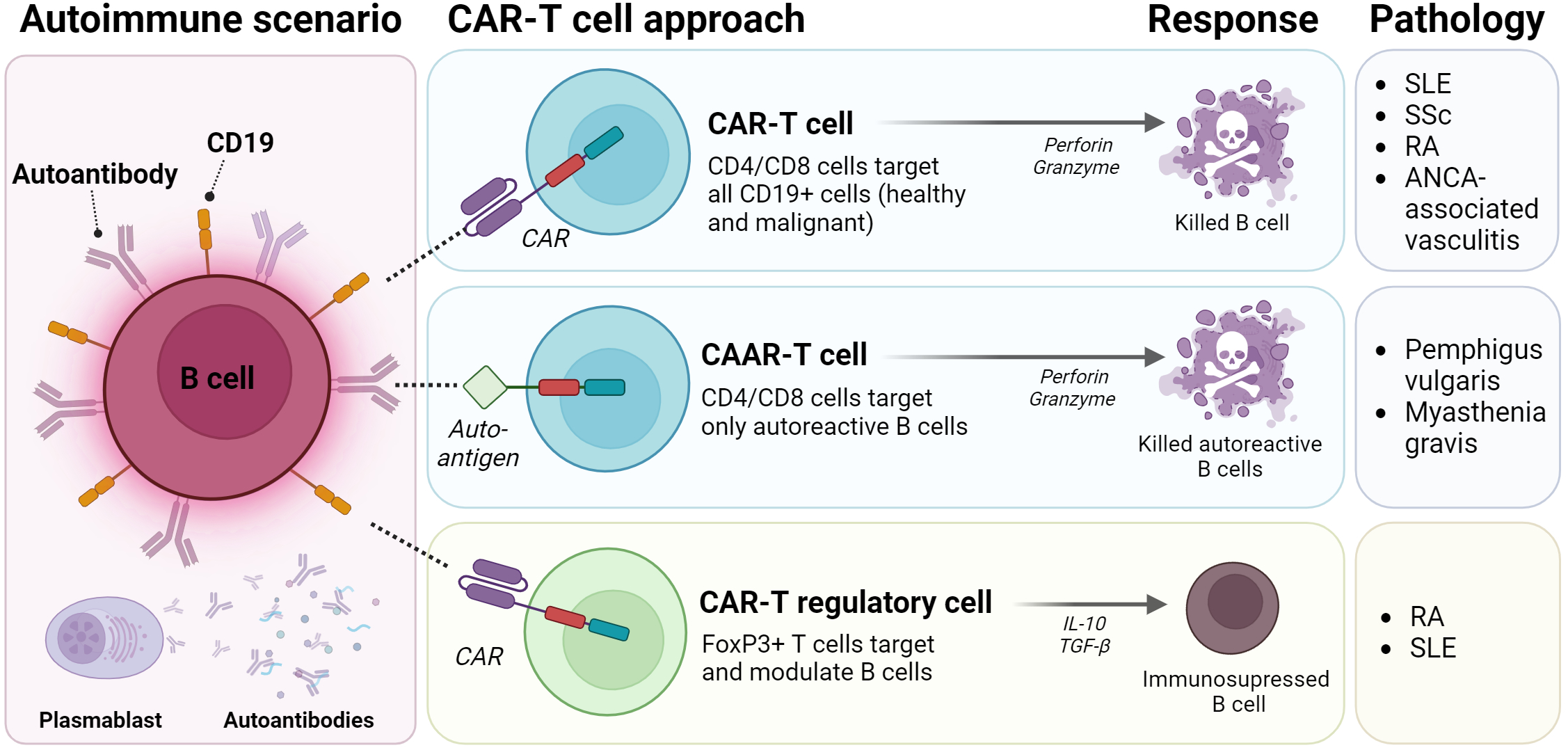
Chimeric Autoantibody Receptor (CAAR) T Cells
– In this modality, the extracellular binding domain of the CAR molecule is replaced with an autoantigen. Binding of autoreactive B cell clones, through B cell receptors (BCRs), to the CAAR in T cells unleashes their cytotoxic activity, leading to specific B cell depletion [1,6,12]. CAAR-T cells were first introduced by Ellebrecht et al. in 2016. The group demonstrated that T cells expressing the autoantigen desmoglein (Dsg) 3 (i.e., Dsg3-CD137-CD3ζ) could kill autoreactive B lymphocytes in vivo in a preclinical model of the antibody-mediated autoimmune disease pemphigus vulgaris (PV) [11]. Currently, CAAR-T cells are being evaluated in clinical Phase 1 and Phase 1/2 trials sponsored by Cabaletta Bio for two indications: muscle-specific tyrosine kinase (MuSK) myasthenia gravis (NCT05451212) and pemphigus vulgaris (NCT04422912).
CAR-T regulatory cells
– This strategy uses T regulatory cells or CD4+ T cells that are modified to overexpress FoxP3 in order to restore immune tolerance. Unlike conventional cytotoxic CAR-T cells, redirected CAR-T regulatory cells exert immunosuppressive functions through various mechanisms, including secretion of anti-inflammatory cytokines (e.g., IL-10 and TGF-β), cytolysis, metabolic disruption, and modulation of antigen-presenting cell maturation or function. Overall, this strategy aims to reduce chronic inflammation associated with autoimmune diseases [1,6,12,13]. Several clinical trials are evaluating CAR-Treg cells in the setting of allogeneic transplantation (cGVHD), including hematopoietic cell transplantation (City of Hope Medical Center- NCT05993611), liver transplantation (Quell Therapeutics Limited- NCT05234190), and renal transplantation (Sangamo Therapeutics- NCT04817774). Significantly, City of Hope Medical Center is also conducting an early-phase 1 study using CD6-CAR-Tregs to target autoreactive effector T cells in patients with type 1 diabetes (NCT07395050). While CAR-Tregs remain at an early stage and challenges remain in their manufacturing and application, they can deliver immune suppression directly to tissues or to antigens driving disease, offering a more precise, tolerance-restoring approach that contrasts with the broad cytotoxic activity of conventional CAR-T cells.
