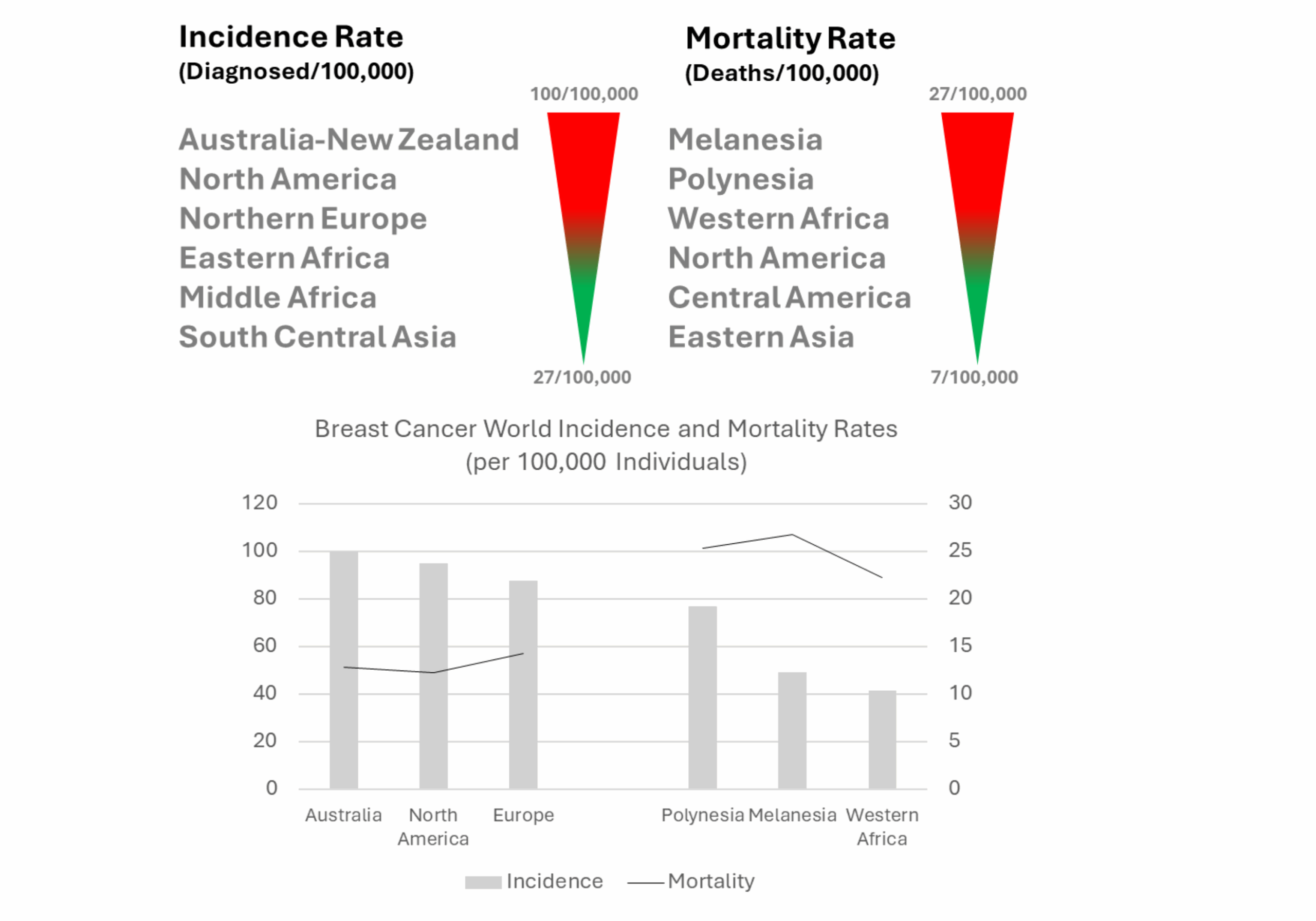
Global Breast Cancer Incidence and Mortality by Human Development Index
Complexity of Breast Cancer Diagnosis and Treatment
Breast cancer is a highly complex and heterogeneous disease, necessitating a multidimensional approach to diagnosis and treatment. Its diagnosis requires histological assessment of tumor type and grade, as well as molecular profiling to define hormone receptor status and the expression of critical proliferation markers. Currently, four main subtypes are defined to guide therapeutic course and disease management, including: luminal A (high expression of estrogen receptor- ER, progesterone receptor- PR, human epidermal growth factor receptor-2- HER2, and Ki67); luminal B (hormone receptor positive, Her2+/-, high Ki67), HER2 overexpressing, and triple-negative breast cancer (TNBC, ER, PR and HER2 negative) [4].
Breast cancer treatment can typically involve various approaches, such as surgery, chemotherapy, radiation, endocrine therapy, targeted therapy, and immunotherapy. Disease management is highly dependent on various factors, including the tumor stage and molecular profile, among others.
For instance, hormone therapy and chemotherapy may be selected for fast-growing luminal B tumors, while in HER2-positive breast cancer, a more targeted approach may be preferred [4].
The Impact of Antibody Drugs in Breast Cancer
Antibody drugs have served as powerful tools in the fight against cancer due to their potential for specific tumor targeting, promotion of anti-tumor immunity (e.g., immune checkpoint inhibitors), disruption of proliferation signaling pathways, and delivery of cytotoxic payloads (e.g., antibody-drug conjugates, ADCs).
The use of checkpoint inhibitors, such as anti-PD-L1 antibodies (e.g., pembrolizumab), has shown efficacy in TNBC. Immune checkpoint inhibitors enhance the body’s ability to fight cancer by lifting natural immune restraints, allowing T cells to mount a stronger attack against tumor cells. Clinical trials have demonstrated significant extension of overall survival when combining pembrolizumab with chemotherapy in patients with metastatic TNBC [4].
Benefits of combining immune checkpoint inhibitors and chemotherapy have also been achieved in patients with early-stage TNBC. Additionally, pembrolizumab and chemotherapy prior to surgery have demonstrated to improve outcomes in patients with HR+/HER2− breast cancer [4].
Antibody drugs directed to HER2 have also led to improved outcomes in HER2+ breast cancer. HER2 signaling regulates cellular growth, survival, and differentiation. In HER2-positive breast cancer, receptor overexpression is common, and therefore, targeting cancer cells with HER2 antagonists serves as an effective strategy to block signaling.

To date, three monoclonal antibodies targeting HER2 have been approved for the treatment of breast cancer. Several clinical studies have investigated the use of anti-HER-2 antibodies in conjunction with chemotherapy or endocrine therapy.
Recent clinical trials suggest that anti-HER2 antibodies, such as trastuzumab, may be effectively combined with endocrine therapy or dual HER2 blockade to reduce reliance on chemotherapy in certain breast cancer subtypes [4].

